
Pre-pectoral breast reconstruction: PU versus ADM
Sie sind bereits registriert?
Loggen Sie sich mit Ihrem Universimed-Benutzerkonto ein:
Sie sind noch nicht registriert?
Registrieren Sie sich jetzt kostenlos auf universimed.com und erhalten Sie Zugang zu allen Artikeln, bewerten Sie Inhalte und speichern Sie interessante Beiträge in Ihrem persönlichen Bereich
zum späteren Lesen. Ihre Registrierung ist für alle Unversimed-Portale gültig. (inkl. allgemeineplus.at & med-Diplom.at)
In immediate pre-pectoral direct-to-implant breast reconstruction, the “interface” choice matters. In this cohort, polyurethane(PU)-coated implants used without acellular dermal matrices (ADM) markedly reduced early seroma and infection and showed lower rates of severe capsular contracture with better long-term aesthetics than total ADM coverage.
Keypoints
-
PU-coated implants without ADM significantly reduced incidence of early seroma (2.9% vs 33.8%) and wound dehiscence (1.4% vs 10.8%) compared with total ADM coverage.
-
The overall complication burden was lower with PU, with more uncomplicated courses and fewer “multiple complication” cases.
-
At 5 years, severe capsular contracture (Baker–Spear grade 3-4) was higher in the ADM group (47.7% vs 24.3%), particularly among non-PMRT patients.
-
Rippling and step-off rates were similar, but blinded aesthetic assessment favored PU for symmetry/position and overall result—supporting individualized technique selection based on flap quality and oncologic variables.
Background
Prepectoral implant-based breast reconstruction following conservative mastectomy (nipple-sparing, skin-sparing, or skin-reducing) has become an established alternative to sub-pectoral placement, with potential benefits in terms of postoperative pain, pectoralis major dysfunction, and animation deformity. In the pre-pectoral plane, the choice of the “interface” between implant and skin flap is pivotal: acellular dermal matrices and polyurethane coating represent two increasingly adopted strategies, supported by different biological rationales and clinical implications.1–7
Study design and surgical protocol
This retrospective cohort study included 97 patients (135 breasts) undergoing immediate pre-pectoral direct-to-implant reconstruction between April 2015 and October 2019. The PU group comprised 70 breasts reconstructed with polyurethane-coated implants (Replicon/Opticon Microthane implants; POLYTECH Health & Aesthetics GmbH). The ADM group comprised 65 breasts reconstructed with textured implants (Polytech Replicon/Opticon POLYtxt; POLYTECH Health & Aesthetics GmbH) fully wrapped with an ADM (Braxon; DECOmed). Outcomes included early (<4 weeks), intermediate (>4 weeks), and late complications (≥1 year), as well as blinded aesthetic assessment using a Likert scale.
Skin-flap perfusion was assessed intraoperatively using indocyanine green (ICG) angiography (Fluobeam; Fluoptics), including early arterial phase, venous phase, and washout, with quantitative analysis of fluorescence intensity. After meticulous hemostasis, sizers were used and contused margins were debrided prior to closure.
Baseline characteristics
A key strength of the study is the standardization of the clinical pathway (predefined time windows for complications, blinded aesthetic assessment, and systematic use of ICG angiography to estimate flap perfusion), which helps mitigate operator-dependent variability and subjectivity in outcome reporting. In addition, follow-up extending to 5 years allows a more robust evaluation of late endpoints, particularly capsular contracture.
Nonetheless, interpretation warrants caution because the two groups were not fully comparable, plausibly also reflecting the sequential adoption of the techniques. Notably, the PU group exhibited a higher rate of postmastectomy radiotherapy (PMRT) compared with the ADM group, representing a potential confounder, especially for long-term outcomes and capsular endpoints.
Early and intermediate complications
Seroma as a clinical “driver”
The most striking finding concerned seroma within 1 month: 2,9% in the PU group versus 33,8% in the ADM group (P<0,001). Early wound dehiscence was also lower with PU (1.4% vs. 10.8%, P=0,029).
Early infection was less frequent in the PU group (1.4% vs 6.2%): all cases were managed with antibiotics; however, in the ADM group one uncontrolled infection required implant removal. Beyond 1 month, infections increased in both groups but remained more frequent in the ADM group (4.3% PU vs. 10.8% ADM).
Regarding overall burden, the PU group more commonly experienced an uncomplicated course (74.3% vs 36.9%); in the ADM group, cases with 3–4 concurrent events were observed, whereas none occurred in the PU cohort (Fig.1).
%20and%20polyurethane%20(PU).jpg)
Fig. 1: Complications in the cohorts with acellular dermal matrix (ADM) and polyurethane (PU)
Red breast syndrome
Red breast syndrome (RBS) was rare and transient in both groups. Marked erythema tended to be more frequent in the ADM group (9.2% vs 1.4%), consistent with the hypothesis that a larger biologically active—and potentially colonizable—surface may predispose to inflammatory phenomena.
Late complications
Capsular contracture at 3 and 5 years
Severe capsular contracture (Baker–Spear grade 3–4) was similar at 3 years (11.4% PU; 12.3% ADM).8 Divergence became apparent at 5 years: 24.3% in the PU group versus 47.7% in the ADM group (P<0.001). Stratified analyses suggested that, within the ADM group, severe contracture occurred predominantly among non-PMRT cases. The authors nonetheless acknowledge the inherent subjectivity of clinical grading and highlight the value of more objective tools (imaging) to compare capsular quality and organization (Fig.2).9
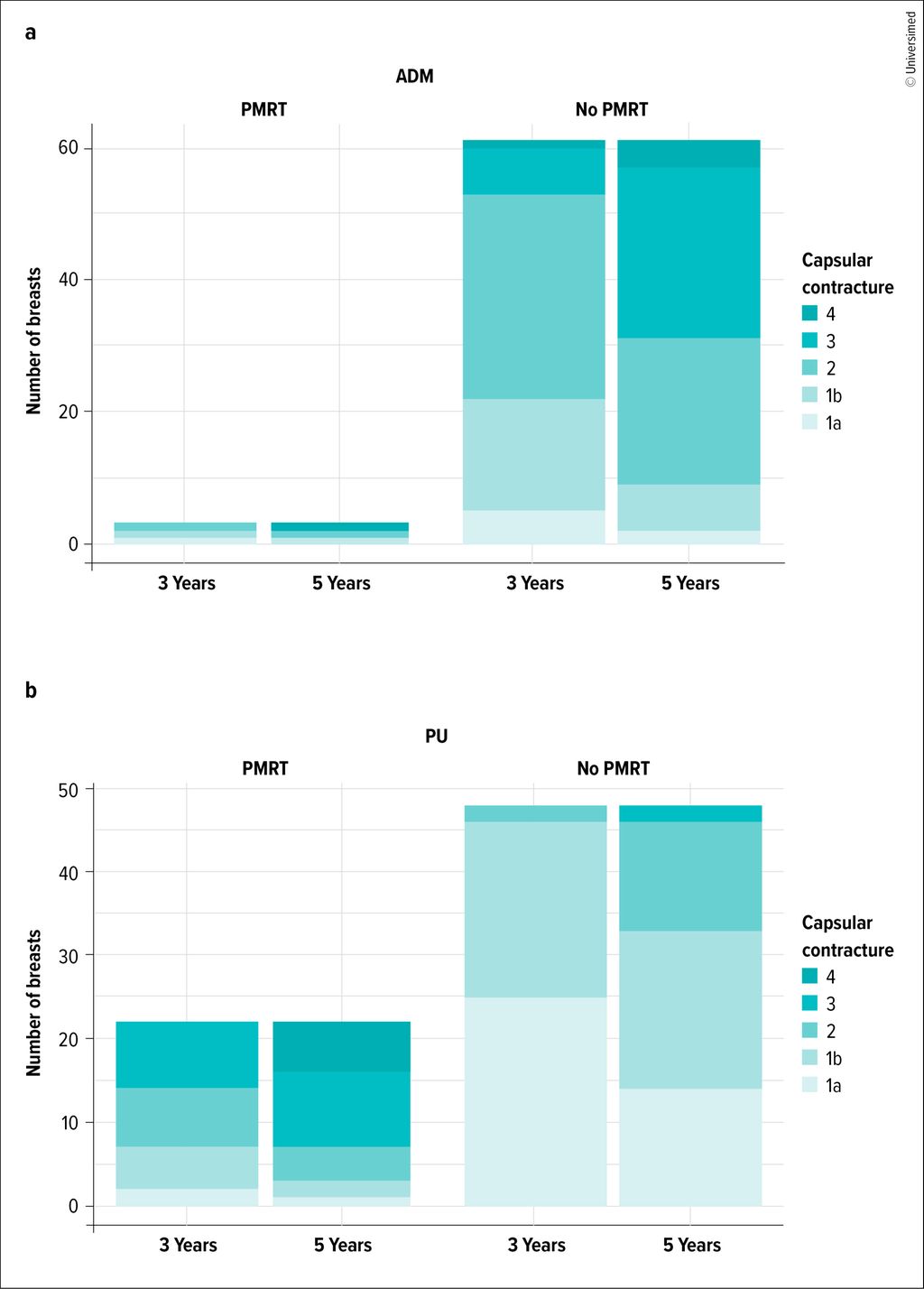
Fig. 2: Graph illustrating the progression of capsular contracture at 3 and 5 years in the acellular dermal matrix group (ADM; a) and in the polyurethane group (PU; b), with and without postmastectomy radiotherapy (PMRT)
Rippling and step-off: minimal differences
Contour deformities did not differ significantly between groups: grade 3–4 rippling occurred in 21.4% (PU) versus 16.9% (ADM), and step-off deformity in 20.0% (PU) versus 21.5% (ADM). No cases of BIA-ALCL were observed.10
Aesthetic outcomes and secondary revisions
Aesthetics were assessed in a blinded fashion using a Likert scale (Fig.3). PU implants achieved higher scores for breast symmetry/positioning and overall aesthetic judgment (P=0.03 and P=0.02, respectively). On multivariable analysis, belonging to the ADM group was associated with a lower likelihood of achieving better aesthetic categories (OR 0.372; 95% CI 0.158–0.856). Overall, 42.3% of cases required minor secondary procedures to refine symmetry and the final result.
%20and%20polyurethane%20(PU).jpg)
Fig. 3: Overall results in the groups with acellular dermal matrix (ADM) and polyurethane (PU)
Proposed mechanistic interpretation
To explain the reduction in seroma, the authors emphasize the adhesive properties of polyurethane (the “Velcro effect”), which may reduce dead space and stabilize the implant by limiting micromotion. In addition, polyurethane coating may retain antibiotic solution more effectively than certain textured surfaces, potentially contributing to differences in infection patterns. While ADM can be advantageous for pocket definition and for masking implant edges, it was associated in this cohort with a higher risk of fluid collections/infections and, long-term, with more severe capsular contracture, as well as potentially longer operative times.
Limitations and practical messages
Key limitations include the retrospective single-center design, non-balanced groups (sequential adoption and baseline differences), and small subgroups (PMRT). Furthermore, the ADM used represented a first-generation product from the manufacturer; therefore, these findings should not be automatically extrapolated to second-generation ADM, for which robust comparative clinical data are still lacking.
Overall, the results suggest that in pre-pectoral direct-to-implant reconstruction, polyurethane-coated implants without ADM may provide a more favorable safety profile (particularly regarding early seroma) and a lower rate of severe capsular contracture at 5 years, with superior global aesthetic outcomes. Device selection should remain individualized based on flap quality, volumes, oncologic variables, and the need for pocket control.
Implications for practice
Polyurethane-coated implants may be preferred when the primary goal is to minimize dead space and seroma events that, in the pre-pectoral setting, can trigger a cascade toward infection, revision surgery, or implant loss. ADM remains a viable alternative, particularly in countries where polyurethane-coated devices are not commercially available, albeit with the acknowledgment of a potentially higher burden of fluid collections and, over the long term, a greater severity of capsular contracture in the cohort analyzed.
Literature:
1 Salgarello M et al.: Direct to implant breast reconstruction with prepectoral micropolyurethane foamcoated implant: analysis of patient satisfaction. Clin Breast Cancer 2021; 21(4): e454-e461 2 Masià J, iBAG Working Group: The largest multicentre data collection on prepectoral breast reconstruction: the iBAG study. J Surg Oncol 2020; 122(5): 848-60 3 Pontes GH et al.: Long-term insights: histopathological assessment of polyurethane implant capsules over 24 years. Aesthet Surg J 2024; 44(9): 915-24 4 Vardanian AJ et al.: Comparison of implant-based immediate breast reconstruction with and without acellular dermal matrix. Plast Reconstr Surg 2011; 128(5): 403e-410e 5 Basu CB, Jeffers L: The role of acellular dermal matrices in capsular contracture. Plast Reconstr Surg 2012; 130(5 Suppl 2): 118S-24S 6 Correia-Pinto JM et al.: Impact of polyurethane versus acellular dermal matrix coating on prepectoral reconstruction outcomes: interface does matter. J Plast Reconstr Aesthet Surg 2024; 91: 15-23 7 de Vita R et al.: Breast reconstruction actualized in nipple-sparing mastectomy and direct-to-implant, prepectoral polyurethane positioning: early experience and preliminary results. Clin Breast Cancer 2019; 19(2): e358-e363 8 Spear SL, Baker JL: Classification of capsular contracture after prosthetic breast reconstruction. Plast Reconstr Surg 1995; 96(5): 1119-23; discussion 1124 9 Mohan AS et al.: Toward a consensus approach for assessing capsular contracture severity and progression: a systematic review. Plast Reconstr Surg 2024; 153(1): 7-22 10 Vidya R et al.: Rippling associated with prepectoral implant based breast reconstruction: a new grading system. World J Plast Surg 2019; 8(3): 311-5
Das könnte Sie auch interessieren:

Medizintourismus für ästhetische Eingriffe und seine Folgen
Günstige Preise und schnelle Termine locken viele Menschen für Schönheitsoperationen ins Ausland. Doch Komplikationen zeigen sich oft erst nach der Rückkehr in die Schweiz – mit teils ...

Lebensqualität durch minimalinvasive funktionelle Gaumenrekonstruktion
Die funktionelle Rekonstruktion im Kopf-Hals-Bereich zählt zu den anspruchsvollsten Aufgaben moderner Chirurgie, da sie zentrale Lebensfunktionen unmittelbar betrifft. Wenn der weiche ...

Einblicke in die Geschichte des Botulinumtoxins
Die Geschichte der Entstehung des Botulinumtoxins ist bemerkenswert: Vom gefürchteten Lebensmittelgift entwickelte es sich zu einem etablierten, weltweit eingesetzten Arzneimittel mit ...